Medical Directors of Clinical Informatics August 2016
August 11, 0730-0830 hours CDT
| Attendees | ||
|---|---|---|
| James Ferrel (Christ) | Christopher Jamerson(Children's) | Mohammed Samee (Illinois Masonic) |
| Anupam Goel (corporate) | Shilpan Patel (Good Shepherd) | Natalie Selk (Christ) |
| Sakhawat Hussain (Trinity) | Douglas Propp (Lutheran General) | Pranjal Shah (Good Samaritan) |
Transcription reduction
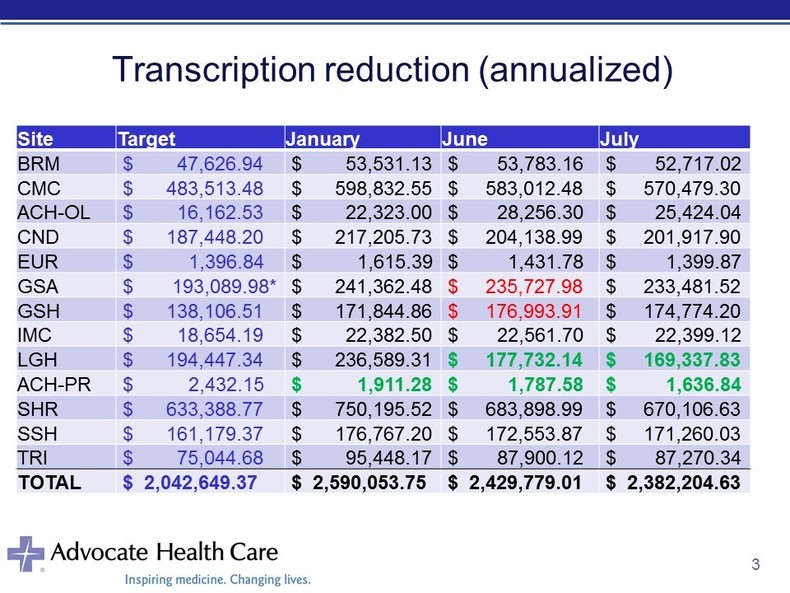
Every site has decreased their transcription costs in July compared to June. The medical directors mentioned two opportunities to improve our physician migration to direct-data entry:
- Differences between telephone transcriptions and direct-entered notes as a barrier that may reduce our ability to move physicians off of transcription. Telephone transcriptions do seem to route to some eClinicalWorks and CliniCare electronic medical records. The functionality for dictated notes does not seem to work for all outpatient practices, but at least some physicians are seeing relevent dictated notes regularly in their electronic medical records.
On a related note, outpatient physicians would like to limited transmitted documents to: history and physicals, consults, operative reports and discharge summaries.
- Many users would benefit from a refresher on using Nuance or PC Touch to enter auto-texts into physician documentation. Rather than spending energy customizing individual user templates, orienting users on how to build common documentation templates to simplify documentation.
CPOE

In the figure above, the red highlights the site's highest peformance in the months displayed. Lutheran has reached its CPOE target for medication CPOE between 8 AM and 5 PM. Our CPOE performance appear erratic from month-to-month. Anupam is still working with the AMG emergency medicine leadership to standardize triage protocols across our sites to remove those orders from this metric's denominator.
CMS recently asked the Office of the National Coordinator to remove any reference to CPOE or computerized decision support from any Meaningful Use incentives or penalties. The medical directors felt that focusing on medication orders from a safety perspective might change physician behavior enought to maintain CPOE expectations for other types of orders (laboratory and radiology). The directors agreed that medication ordering represents a safety priority and physician accountability. Each handoff between users represents an opportunity to miscommunicate.
Leadership interest in mandating physician EMR education
Based on feedback from this group and others, a physician education proposal now includes the following elements:
- Initial session after obtaining hospital credentials: orientation with some specialty-based optimization
- Follow-up session two-four weeks after working with CareConnection: second session with additional optimization based on user-specific workflows
- Regular follow-up sessions every six-12 months
The group would like to link the follow-up sessions with some sort of proficiency testing or tracking against EMR metrics (e.g., transcription costs, CPOE). Some education might focus on sharing best practices acquired from watching our best performers to share with others.
DIRECT
[] Pranjal will reach out to the Nephrology group at Good Samaritan to see if they would be willing to try this workflow using NextGen.
[] The Best Practices hospitalist group would be interested in testing this functionality with their outpatient colleagues.
Revenue Cycle Update
Anupam updated the group on Advocate's roadmap to deploy Cerner's Revenue Cycle functionality by early 2018. From a physician perspective, the elements Anupam is supporting is moving to a single physician directory and updating workflows that cross care settings (e.g., pre-operative H&Ps prior to day surgery). The group expressed the following concerns:
- The organization under-invests in registration staff on the front end, leading to cascading errors throughout the patient's hospital stay and beyond.
- What is Advocate's interest in self-registration kiosks like the airports? Since the meeting, Anupam has learned AMG is investigating that workflow for our Walgreens clinic locations.
- Has Advocate considered linking registration to the patient's portal account?
- How many data elements will be present in the provider directory to unambigously identify a single physician?
- How will the new registration process help end-users appropriately select the correct encounter (i.e., FIN) when a patient has multiple encounters?
[] Anupam to discuss these concerns with the Cerner Revenue Cycle team when he meets with them.
Issues from prior meetings
[] Doug's request to identify capitated patients on the ED - a system workgroup has identified a process to notify emergency department users that the patient is a "covered life." The functionality should go live sometime in the next four-six weeks.
[] If the signature + specialty request (with changing the resident's specialty with each rotation) and SmartTemplate work are performed by separate teams, then we will proceed down both paths simultaneously. Otherwise, we will work on the SmartTemplate request first before adding troponin in the daily labs SmartTemplate.
[] Anupam is still waiting to hear back from the Advance Care Planning Council about changing the requirement for a physical signature for LET orders.
The next meeting is scheduled for September 8, 2016.
Advocate Physician Informatics
Increasing physician knowledge and proficiency with Advocate Health Care's clinical information systems.
